The bladder stays healthy by continually filling and emptying. Your bladder is a storage organ, it gradually fills many times during the day.
The pelvic floor muscles contract and the bladder sphincter keeps the bladder tube (urethra) closed so wee is stored. You may first recognise you need to go to the toilet when it is holding around 150ml, but we often ignore these first signs. Generally, people visit the toilet to pass wee when it is convenient, and the bladder is holding approximately 400mls of wee. If we drink regularly throughout the day around 1.5-2 litres (recommended daily amount), we visit the toilet between 5-8 times a day.
When we pass wee the bladder squeezes, the pelvic floor muscles and the bladder sphincter relaxes to allow the wee out. There should be a good flow, a feeling of compete emptying and no dribbling after you have left the toilet.
There are several things that can affect bladder health, these include:
· Difficulty finding or accessing a toilet regularly, meaning you are having to hold on or going to the toilet ‘just in case’ and go to soon.
· Not Drinking regularly throughout the day. Drinking water is best up to 1.5-2litres, try to avoid caffeinated or fizzy drinks as this can irritate the bladder.
· Avoiding constipation as this can put stress on the bladder especially if you are straining.
· Not having your fleet flat on the floor when having a wee. This can cause the pelvic floor to not fully relax when emptying.
· Urine infections.
Click on the link here for more information on management techniques.
(Please note UHNM does not take responsibility of accessibility of external websites and documents)
Good Bowel function is important to feeling healthy; when things aren’t working well it very quickly influences our quality of life
It is normal to open your bowels (have a poo) between three times a day, to three times a week. Every bowel function is individual and varies with many factors, such as diet, fluid, lifestyle and age. We should be able to:
1. Have an awareness of the need to open our bowels. 2. Hold on to go to the toilet at an appropriate place and time. 3. We should be able to open our bowels completely, without straining when we sit on the toilet.
Ideally, we don’t want to be constipated but we also don’t want to experience bowel leakage (incontinence).
Constipation
It's likely to be constipation if:
you have not had a poo at least 3 times during the last week or you're pooing less often than usual
the poo is unusually large or small and is dry, hard or lumpy
you are straining or in pain when you have a poo
you feel like you haven't fully emptied your bowels
Remember-Do not strain on the toilet!
Sit fully on the toilet: do not ‘hover’
Have your feet apart and raised up on a stool/ support, ideally with knees over hips in a squatting position, with your arms resting comfortably on your legs.
Keeping your tummy relaxed; don’t tighten your abdominal muscles
Avoid breath holding; try to have a relaxed breathing pattern, breath out when you feel like pushing, think of Moo to Poo
It is also important to eat a healthy balanced diet which includes fibre, exercise little and often and drink plenty of water
Bowel incontinence
You might have bowel incontinence if you cannot control when you poo. Symptoms of bowel incontinence include:
• poo leaking out without you being able to stop it • feeling like you need to poo, but not being able to get to the toilet in time • not being able to get fully clean after going to the toilet
Poor pelvic floor muscles can make it difficult to hold on when you need to go to the toilet.
Optimal consistency of your poo should be around type 4 on the Bristol Stool Chart below. It should be firm but not hard and easy to pass without the need to strain.
See below useful information regarding your bowel health:
For most women, it is safe to exercise and actively encouraged during pregnancy. There are some conditions where exercise may not be encouraged or consent from GP/midwife must be given. It is always best to check with your care giver if you have any queries.
In pregnancy, the aim should be to maintain or moderately improve your level of fitness. After your baby is born the aim is to regain the former level of fitness, or to improve on it.
Moderate exercise intensity is also known as the Talk Test – you should be able to carry on a conversation while exercising.
Lying flat on your back after 19 weeks of pregnancy or front lying once your bump is showing should be avoided. This is due to the extra pressure it places on the joints and ligaments in your spine, as well as the changes in blood flow that occur as pregnancy progresses.
Advantages of exercise:
• an increased release of endorphins (your body’s ‘feel-good’ chemicals) • helping to improve your sleeping pattern • improvement of your balance and posture • maintaining a healthy body and mind • helping to control your weight • helping in the prevention of pregnancy induced diabetes (Gestational Diabetes Mellitus or GDM), • helping your body prepare for labour and delivery • increased fitness levels and quicker recovery after childbirth If you’re not active, start gradually. If you’re already active, keep going.
This can be achieved: • at home • during leisure • out and about
Examples of moderate intensity physical activity include:
• climbing stairs • yoga • swimming • gym activities (such as using the treadmill) • carrying grocery shopping bags • cycling • dancing • going for a walk
Feelings of anxiety during pregnancy, labour and while adjusting to life as a parent are very common. The art of relaxation is a valuable skill to learn to help cope with challenges of pregnancy, birth and life with your baby. Keeping relaxation exercises simple and practicing often helps you quickly master skills.
Deep abdominal breathing is the most efficient method of breathing for you and your baby and helps relax. This technique assists you to relax and begin preparing for birth. Why to do it: Deep diaphragmatic breathing (abdominal breathing) is a helpful technique for dealing with pain, anxiety, stress. It helps you to relax, acts as a distraction and reverses some of the physical symptoms of anxiety. How to do it:
Many people, especially when they are upset, stressed, anxious, or in pain breathe only from the upper part of their chest. Instead, try taking slow, deep breaths from the abdomen. Rest your hands along the bottom of your ribcage, so that the fingertips of each hand are just touching. Your fingertips should move apart slightly as you breathe in, and then come together again as your lungs empty. Breathe slowly, for example for a count of 5 in through your nose, and breath out equally as slowly out through your mouth, this ensures the diaphragm is pulling air into the bases of the lung.
The Pelvic floor muscle forms a sling from the front (pubic bone) to the back (tail bone) of your pelvis and support the organs within it. They also play a role in controlling your bladder, bowel and sexual functions.
Pregnancy can put extra strain on your pelvic floor muscle as it supports your growing baby during pregnancy and stretches during labour. Having strong pelvic floor muscles means you’ll be less likely to have issues like stress incontinence after your baby is born.
This can include:
Leaking when coughing, sneezing, lifting or running.
Less sensation when having sex.
Reduced control over passing wind.
A prolapse which is where one or more of your organs can press against the vaginal wall causing a bulge.
Evidence shows completing your pelvic floor exercises can help to reduce the risk of developing the above symptoms.
Pelvic floor exercises:
Pelvic floor muscle training:
The correct way to contract your pelvic floor muscles is tighten from back to front as if you’re trying to stop wind and wee.
You need to be able to draw those muscles upwards and forwards from the back passage towards the bladder. Imagine a plane taking off or an elevator rising.
You can do these exercises lying down, sitting or standing. With practice, they can be done anywhere and at any time:
Pelvic floor exercise programme:
There are two types of squeezes to do:
Long squeezes:
Tighten your pelvic floor muscles as described above, keep holding them tight, then release
and let them fully relax, think of it like turning up a dial. Make sure you breathe normally throughout keeping all other muscles relaxed.
How many seconds or how many breaths in and out can you hold the squeeze?
Repeat the long squeezes, with a rest in between, until the contraction isn’t as strong or you can't feel the muscle relax.
How many times can you repeat the squeezes?
Quick squeezes:
Quickly tighten your pelvic floor muscles, then immediately let them go again. Think of it like a switch.
How many times can you do this quick squeeze before the muscles get tired?
Always let the muscles fully relax after each squeeze. If you can’t feel the muscles relax then the chances are the muscles have become tired.
How many am I aiming for?
Long squeezes: the aim is to work up to 10 second holds, repeated ten times.
Quick squeezes: contract for one second, relax for one second and repeat this up to 10 times.
Complete the above 3 times a day. Slow squeezes followed by fast squeezes make up a ‘set’. You should notice an improvement in 3-5 months
It's important to keep breathing normally while you do these exercises. Make sure you do not pull in your stomach when you squeeze. When breathing in, breath in through your nose out through your mouth.
Once you’ve achieved this and your symptoms have resolved, you can drop down to once per day or three times per week for life-long maintenance.
In everyday life you may find the Knack technique helpful.
The knack technique is when you tighten your pelvic floor muscles before and during certain activities to reduce strain on your pelvic floor muscles and prevent leakage of wee are poo. You should use this technique when you: cough, sneeze, laugh or picking something up.
It is easy to forget to do your pelvic floor exercises, it can help to do them at the same time every day, or time them with mealtimes. Setting alarms or reminders on your phone or using the squeezy app can be helpful.
Pelvic floor dysfunction (PFD) is used to describe conditions that are caused by the pelvic floor muscles not working as they should.
Symptoms can include:
• Urinary incontinence - leaking of wee. • Urge incontinence - urgency to wee more than seven times a day. • Anal incontinence – leaking of poo or wind. • Pelvic organ prolapse - one or more of the pelvic organs start to come down into the vagina. • Pain or discomfort during sex.
Pelvic floor dysfunction can be common, but they do not have to be your new normal and it should not be accepted that it’s a normal part of pregnancy and giving birth. Symptoms can occur but should only last for a short time and should be mild.
The most common symptom to experience during pregnancy and after birth is urinary incontinence (leaking wee).
• It occurs in around 40 to 50 per cent of women and birthing people as pregnancy progresses and immediately after birth. • Around 25 per cent of pregnant women and birthing people can also have anal incontinence (leaking poo). Please complete the self-referral form on our home page if you like further support with your symptoms
The most common type of incontinence is stress incontinence. It is caused by physical stress on your bladder that can make you leak wee. It often happens when you cough, sneeze or exercise. Common causes include weakened pelvic floor muscles, examples include pregnancy and childbirth.
Urge incontinence
Urge incontinence is when you feel a sudden and very intense need to pass wee and you are unable to delay going to the toilet. There are often only a few seconds between the need to urinate wee and the release of urine. There can be several reasons as why this happens for example drinking fluids that can irritate your bladder such as caffein and fizzy drinks.
Management is key. This can include good bladder and bowel habits, making lifestyle changes and pelvic floor exercises
You might have bowel incontinence if you cannot control when you poo. Symptoms of bowel incontinence include:
• poo leaking out without you being able to stop it • feeling like you need to poo, but not being able to get to the toilet in time • not being able to get fully clean after going to the toilet Management is key. This can include good bladder and bowel habits, making lifestyle changes and pelvic floor exercises
Prolapse is common affecting 1 in 12 people. Normally the pelvic organs (bladder, bowel, uterus and vagina) are supported in our pelvis by ligaments, fibrous tissue and the pelvic floor muscles. A prolapse occurs when one or more of these organs slips or bulges down towards the vagina due to weakness of the pelvic structures. Causing the feeling of ‘something coming down’ or vaginal heaviness or a dragging feeling. The bulge might be felt inside or outside the vagina. Prolapse can cause bladder, bowel or sexual symptoms. Having a prolapse can also affect how your bladder and bowel function and can also make sex uncomfortable.
There are different types of prolapse, its common to have more than one type of prolapse at the same time.
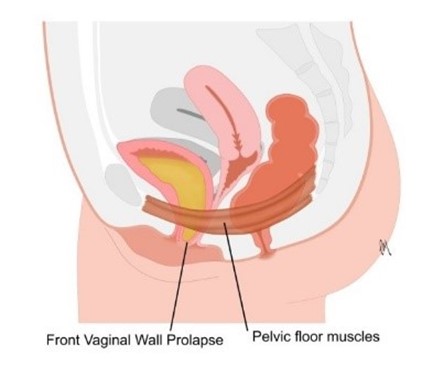
Front vaginal wall (cystocele)
This is the most common. The wall supporting the bladder bulges down. This can cause problems with emptying the bladder, causes frequent urine infections, increases how desperately you need to empty your bladder (urgency).
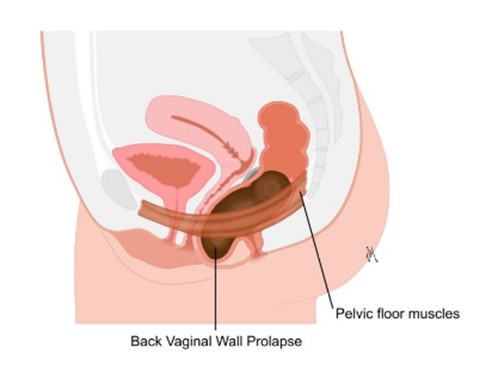
Back vaginal wall prolapses (rectocele)
The wall supporting the rectum bulges down into the vagina contributing to bowel symptoms. This can cause symptoms such as difficulty emptying the bowel, controlling wind and the speed that you need to go to the toilet.
Uterine prolapse
Uterus moves down towards the cervix. Symptoms might include feeling something coming down. It can often be felt or seen with a mirror. It might be uncomfortable inserting tampons, obstruct sex and cause pain or discomfort.
Risk factors of prolapse include pregnancy, childbirth, being overweight, heavy lifting, age, family history, constipation, cough, previous pelvic surgery.
Management is key:
This can include good bladder and bowel habits, making lifestyle changes and pelvic floor exercises
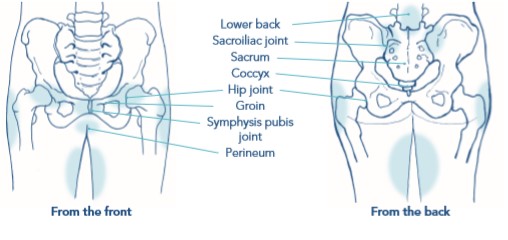
Some women or birthing people may develop pelvic pain in pregnancy. This is sometimes called pregnancy-related pelvic girdle pain (PGP) or symphysis pubis dysfunction (SPD).
Pregnancy related pelvic girdle pain (PGP) is common, but it is not normal or expected during pregnancy. PGP describes any pain that you feel around your pelvis.
You may find it difficult to walk, taking weight on one leg, pain when separating your legs and clicking or grinding of the pelvis.
We used to think it was down to increase in the hormone relaxin making the joints loose, this is no longer the case. Your pelvis remains strong throughout pregnancy.
When you experience pain, it does not always mean the pelvis is ‘damaged’. Pain and emotions are processed in the same part of the brain. There are a lot of changes that happen during pregnancy which naturally heightens the nervous system. It can make the body behave in a protective way, it can mean the muscles feel tight and movements can feel difficult, restricted or painful. This can last longer than it should do and can lead to a sensitised nervous system.
See below for more information on how to improve your PGP: including management, how physiotherapy can help your symptoms, exercises, positions of ease during pregnancy and labour and after baby arrives.
If you have symptoms lasting more than two weeks, or interferes with normal day to day life let your midwife know or use the self- referral link on the home page.
If you have symptoms lasting more than two weeks, or interferes with normal day to day life let your midwife know or use the self- referral link on the home page.
(Please note UHNM does not take responsibility of accessibility of external websites and documents)
Click here to watch the Reducing severe tears animation
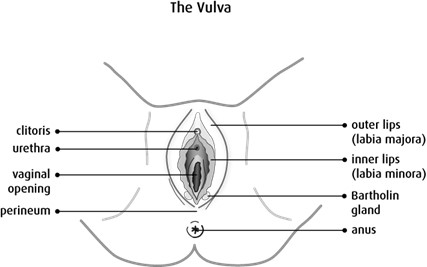
Your perineum is the area between your vaginal opening and back passage (anus).
It is common for the perineum to tear to some extent during childbirth. Tears can also occur inside the vagina or other parts of the vulva, including the labia.
Up to 9 in every 10 first time mothers who have a vaginal birth will experience some sort of tear, graze or episiotomy. It is slightly less common for mothers who have had a vaginal birth before.
For most women, these tears are minor and usually heal quickly.
The good news is there are ways to reduce the risk of having a severe tear.
If you wish to discuss any aspects of this section, please contact our Specialist Pelvic Health Midwife or you can use the self-referral link on the homepage.